

Abstract
Background: Transplant associated thrombotic microangiopathy (TA-TMA) is a well-recognized complication of hematopoietic cell transplantation (HCT) and in a pediatric cohort, a prevalence rate of 39% is reported (Jodele, et al 2016). However, TA-TMA is challenging to diagnose as features are common to and may occur concurrently with many post HCT complications, i.e. acute graft versus host disease (aGVHD) and infection. Outcomes are historically poor, though it is unclear if this is secondary to TA-TMA or to concurrent morbid conditions. We aimed to describe the prevalence and outcomes of TA-TMA at a single large pediatric center.
Methods: In this retrospective study, data were extracted from the medical records of all children who received an HCT at Boston Children's Hospital from 1/2015-08/2017. Records were reviewed for evidence of TA-TMA in the first 100 days after HCT. According to "probable diagnostic TA-TMA criteria" (Cho et al, 2010), all the following had to occur concurrently and during at least 2 consecutive time points: 1) elevated lactate dehydrogenase, 2) platelet count <50 × 109/L or a ≥50% decrease, 3) anemia or requiring transfusions, 4) schistocytes in the peripheral blood, and 5) absence of a coagulopathy and a negative Coombs test. Patients who were both clinically diagnosed and retrospectively met criteria for TA-TMA were grouped together for analysis. Fisher's exact test (categorical variables) and Wilcoxon rank-sum test (continuous variables) were used for comparison. Kaplan-Meier curves were generated for overall survival (OS). All non-relapse deaths were considered transplant-related (TRM). Competing risk analysis was performed using Gray's test. Multivariable competing risks analysis was performed using a proportional hazards model for TRM.
Results: 275 HCTs were performed in 232 patients. Among allogenic transplants (n=163), cell source was largely bone marrow (87%). Median follow up time of survivors was 1.3 years (range 0.04-2.9 years). Thirty-seven patients (16%) met criteria for TA-TMA; 6 were clinically diagnosed and 31 retrospectively met criteria. TA-TMA was diagnosed a median of 26 days (range 11-97 days) after cell infusion. Patients who met criteria for TA-TMA had significantly higher rates of aGVHD, ICU admissions, engraftment failure, bacterial and or viral infections in the first 100 days and were more likely to have an unrelated donor HCT, an HLA-loci mismatch of <10/10, and ³2 HCT (p<0.05). There were no differences in age at HCT, cell source, sex and HCT indication.
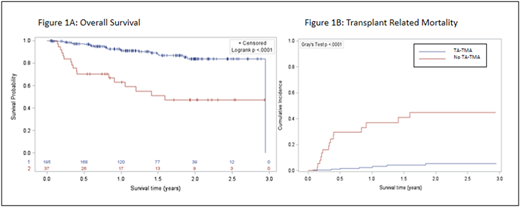
OS was significantly lower in patients with TA-TMA, with a one-year OS of 63.1% (95% CI=46.8-79.3%) vs 92.1% (87.9-96.2%), (log-rank p<0.0001; Figure 1A). TRM was significantly higher both at 100 days 16.2% (6.5-29.9%) versus 2.4% (0.8-5.6%), and one year 37% vs 2.4%. (Gray's test p<0.0001; Figure 1B). In a multivariable model adjusting for the development of grade 4 aGVHD (Hazard ratio [HR]=4.4, 95% CI=1.2 - 15.7, p=0.02) and engraftment failure (HR=2.1, 95% CI=0.4-9.9, p=0.4), the risk of TRM was significantly higher when screening positive for TA-TMA (HR=9.1, 95% CI=3.2-25.8, p<0.0001).
Of the 6 patients diagnosed with TA-TMA by providers, 4/6 were treated with eculizumab; 2 died of multiorgan failure and 2 remained dependent on eculizumab for ³2 years to maintain control of disease. The other 2 patients had aGVHD prophylaxis switched from cyclosporine to a different agent, resulting in TA-TMA resolution. TRM at 1 year was 33%. Of the 31 patients who retrospectively met criteria none received TA-TMA directed therapy. All were treated for the primary condition at the time of positive screening: aGVHD (n=9), engraftment failure (n=4), infection (n=6), multiorgan failure of unclear etiology (n=2) and other (n=16). One-year TRM was 38.2%.
Conclusion: The prevalence of TA-TMA at our institution is 16%, lower than other reports using the same diagnostic criteria. 83% (31/37) of patients who met criteria for TA-TMA were retrospectively identified while being treated for another transplant complication, highlighting the challenge of a clinical diagnosis in the setting of non-specific criteria. Patients with TA-TMA had worse overall survival and increased TRM, even when adjusting for the development of aGVHD and engraftment failure (HR 9.1). It is important to develop multi-institutional, prospective studies to identify risk factors for TA-TMA and further study therapies and outcomes.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal